![[Chronicle]](/images/sidebar_header_oct06.gif)
Vol. 23 No. 11
Drug to treat hepatitis B proves useful in blocking anthrax toxin
By John EastonMedical Center Public Affairs
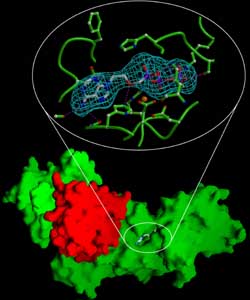 The upper part of this image shows a structural model of the active form of adefovir as it interacts with the edema factor-calmodulin complex (green). The lower part of the image shows adefovir bound to the “pocket” on the complex of edema factor (green) and calmodulin (red). | |
Researchers at the University have found that a drug approved in 2002 to treat chronic hepatitis B can block the action of an anthrax toxin.
In the online edition of the Proceedings of the National Academy of Sciences, a team led by Wei-Jen Tang shows that in vitro, the drug adefovir dipivoxil effectively reduces the effects of edema factor, one of the two deadly toxins produced by anthrax.
“These toxins pack a one-two punch that makes inhalational anthrax extremely harmful,” said Tang, Associate Professor in the Ben May Institute for Cancer Research at the University. “For the first time, we have a clinically approved drug that, at least in tissue culture, completely eradicates half of that toxic team, and does it at non-toxic doses.”
Until the fall of 2001, Bacillus anthracis, the bacterium that causes anthrax, was considered an obscure agricultural pathogen with a few interesting properties. But in the fall of that year, someone began sending threatening letters stuffed with anthrax spores to several politicians and journalists.
Nearly half (5/11) of those infected by breathing in the spores died from the disease. Many of those who survived have ongoing symptoms such as fatigue, shortness of breath and memory loss. “This highlights an urgent need,” noted the authors, “for a more effective treatment.”
The anthrax mailings triggered a run on the antibiotics that are used to treat the infection, but which are only effective in treating the early stages of anthrax infection, before the bacteria have had time to spread and secrete their antibiotic-resistant toxins.
These toxins, edema factor and lethal factor—as well as a molecular escort called protective antigen that helps the toxins enter cells—are what make this microbe so deadly.
In the early stages of an infection, edema factor interferes with the host’s immune response, allowing the bacteria to spread, multiply and produce more toxins. Later, edema factor causes massive tissue damage, including the release of fluid into the lungs as well as the formation of the blackened necrotic lesions that give the disease its name (from Greek anthrakos, meaning “coal”).
In January 2002, Tang’s lab published a paper in Nature that described the three-dimensional structure of edema factor and showed how it causes its effects by hijacking a normal cellular process and forcing it into overdrive. Because of the bioterrorist attacks a few months before, Tang’s discovery received widespread media attention.
A researcher who works with the drug saw newspaper accounts of Tang’s research and wondered if adefovir acted on the same metabolic pathway. He contacted Tang and eventually sent him several candidate compounds, including adefovir dipivoxil.
Adefovir was designed to inhibit an enzyme used by the hepatitis B virus to make copies of itself. Researchers in Tang’s lab found that the active metabolite of adefovir also blocks edema factor, preventing it from interfering with the host’s immune response and eradicating its toxic effects.
Using the Advanced Photon Source at Argonne National Laboratory, Tang’s team was able to determine the precise structure of the active form of the drug bound to its target, which revealed how it neutralized edema factor.
In earlier work, Tang showed that edema factor, inside an infected cell, connects with a protein called calmodulin. Calmodulin changes the toxin’s shape, creating a conformation that functions similar to a cellular enzyme called adenylyl cyclase, which helps regulate cell-to-cell signaling.
When edema factor connects with calmodulin, however, it becomes a relentless version of adenylyl cyclase—1,000-fold more potent—causing affected cells to become hyperactive. These cells devour their energy stores, lose the ability to regulate their environment, release water, causing edema (swelling) in surrounding tissues, and die.
Tang found that adefovir fits neatly into a pocket on the surface of edema factor in a way that prevents it from mimicking adenylyl cyclase. In fact, adefovir fits the pocket 10,000 times better than its natural substrate does Remark-ably, adefovir’s affinity for edema factor is four times greater than its attraction to the hepatitis B virus enzyme it was designed to inhibit.
Because the drug is such a precise match to its target, it may require only small amounts of adefovir to effectively block edema factor. Such small amounts should produce few, if any, side effects in short-term use for anthrax.
How much difference adefovir might make in treating inhalational anthrax in humans is still untested. Although anthrax makes two toxins, they work together. Mice infected with a strain of anthrax that makes only lethal factor and not edema factor are 100 times more likely to survive.
“The two toxins and protective antigen all multiply each other’s effects,” explained Tang, “so blocking any one of them should have a major impact.”
Tang’s studies suggest that adefovir may also inhibit similar toxins produced by more common disease-causing bacteria including: Bordetella pertussis, which causes whooping cough; Yersinia pestis, which causes plague; and Pseudomonas aeruginosa, a common cause of hospital-acquired infections and a scourge for patients with cystic fibrosis. All three also are considered potential bioterror agents.
“We all hope that the bioterror attacks of 2001 never recur,” said Tang, “but if something happens, it would be nice to have better treatment options.”